Every human being is the author of his own health or disease.
– Gautama Buddha
SYNOPSIS
Pelvic Inflammatory Disease (PID) is an infection of the female reproductive organs. It is caused by many types of bacteria. If not treated, it can cause complications such as ectopic pregnancy and infertility.
PID affects women in reproductive age. Peak incidence is in women of 15 to 24 years age. India is estimated to have at least one million episodes of PID each year.
Risk of PID increases with risky sexual practices: multiple sexual partners, sex with a person having PID, starting sex at a very young age and having sex without a condom.
PID often has no signs or symptoms. But a few of the symptoms that may appear are: pain in lower abdomen or pelvic pain, heavy or foul periods, bowl discomfort and pain in urination.
There is no single test to diagnose PID. It is diagnosed from symptoms and from gynaecological examination. Urine and blood tests, ultrasound, and laparoscopy may also be used. Because of absence of symptoms, and because the symptoms are similar to those of other diseases, PID diagnosis is often delayed. Woman’s recent sexual partners also need to be tested and treated.
A mixture of antibiotics is used for treatment and is successful in most cases. But a few cases may need laparoscopic or surgical intervention. Removal of intrauterine devices (IUDs) is not necessary.
Because of difficulty of diagnosis, and serious consequences of delayed treatment, empirical treatment may be initiated in at-risk women if symptoms of PID appear. Having regular medical care throughout lifetime maximizes the chances of early diagnosis and treatment of PID.
Improved education, routine screening, diagnosis, and empirical treatment of PID will reduce the incidence and prevalence of PID and its long-term sequelae.
INTRODUCTION
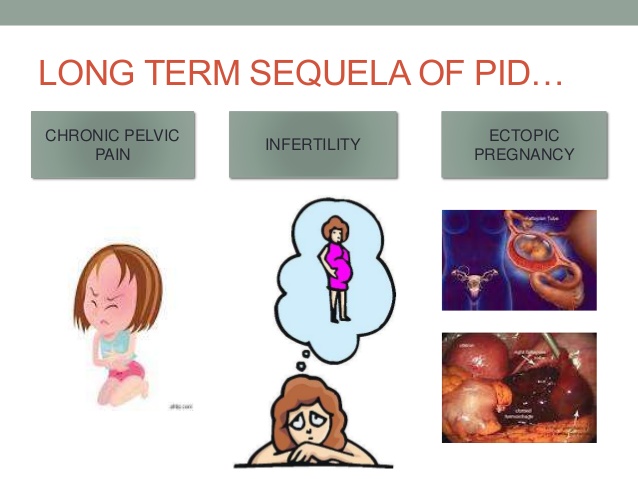
PID, if not treated, can cause ectopic pregnancy, infertility, chronic pelvic pain, cancer, peritonitis and tubo-ovarian abscess – the latter two can become life threatening.
In the US, more than one million women have PID, and more than 100,000 become infertile each year because of PID. In industrialized countries PID-incidence is 10 to 13 per 1,000 in women in 15 to 39 years age-group, with a peak incidence of about 20 per 1,000 women in 20 to 24 years age group. India is estimated to have more than one million PID episodes each year.
CAUSE
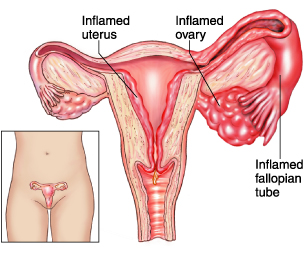
PID is an infection of the female reproductive organs – vagina, uterus, fallopian tubes, ovaries, and of womb lining (endometrium) and lining of the inside of the abdomen (peritoneum).
It is a bacterial infection. Many types of bacteria can cause it but in about one in four cases it is caused by sexually transmitted infection (STI) such as chlamydia or gonorrhoea. Sometimes normal, harmless, bacteria in the vagina get past the cervix and into the reproductive organs and cause PID. This can happen when the cervix is damaged after childbirth, miscarriage, abortion and inspection of the womb; or by an earlier PID.
In many cases, the cause of PID is unknown.
RISK FACTORS
Any woman can get PID. But the risk of getting it is increased by:
• Being sexually active and younger than 25 years age
• Having multiple sexual partners
• Having a new sexual partner
• Being in a sexual relationship with a person who has more than one sex partner
• Having a history of PID or STI
• Having sex without a condom
• Douching regularly, which upsets the balance of good versus harmful bacteria in the vagina and might mask symptoms
Having an intrauterine device (IUD) does not increase the risk of PID. Potential risk, if any, is within the first three weeks after insertion.
SYMPTOMS
PID often has no signs or symptoms. But one or more of these symptoms may occur:
• Pain in lower abdomen
• Pelvic pain — especially during a pelvic exam
• Heavy or foul or painful periods with an unpleasant odor
• Unusual vaginal discharge, especially if it’s yellow or green
• Abnormal uterine bleeding, especially during or after intercourse, or between menstrual cycles
• Pain or bleeding during intercourse
• Fever, sometimes with chills
• Painful or difficult urination
• Bowel discomfort
• Nausea and vomiting
See your doctor if you experience any of the above symptoms.
Vaginal discharge with an odor, painful urination or bleeding between menstrual cycles can be associated with STI. If these signs and symptoms occur, stop having sex and see your doctor soon. Prompt treatment of an STI can help prevent PID.
DIAGNOSIS
There is no single test to diagnose PID. It is diagnosed from symptoms and from gynecological examination.
Gynecologist in Delhi will talk about your medical and sexual history and do a pelvic examination to check for any tenderness and abnormal vaginal discharge. This examination may be discomforting, especially if you have PID.
Swabs may be taken from the inside of your vagina and cervix to look for bacterial infection and identify the bacteria responsible. A positive test for chlamydia or gonorrhoea supports the diagnosis of PID. Most women test negative but this does not rule out PID.
Other tests may, therefore, be required to look for signs of infection or inflammation, or to rule out other possible causes of your symptoms. These tests may include:
• a urine or blood test
• a pregnancy test
• an ultrasound scan, which is usually carried out using a probe passed through the vagina (transvaginal ultrasound)
In a few cases, especially the more severe cases, and where there may be other possible causes of the symptoms, such as appendicitis, laparoscopy may be used to look at the internal organs and, if necessary, take tissue samples to diagnose PID. Laparoscopy can also be useful in disproving cases wrongly labelled as chronic pelvic disease.
Recent sexual partners also need to be tested and treated to stop the infection recurring or being spread to others.
Diagnosis of PID can be missed or delayed because of absence of symptoms in the earliest, most curable stage. When symptoms do occur, they can be similar to symptoms of certain other diseases, such as appendicitis, food poisoning or food borne illness, ruptured ovarian cyst, diverticulitis, and ovarian torsion. Therefore have regular medical care throughout lifetime to maximize the chances of early diagnosis and treatment of PID.
TREATMENT
If diagnosed early, PID is treated with antibiotics for 10-14 days. A mixture of antibiotics to cover the most likely infections is given as tablets and injections. Complete the antibiotic course and avoid sexual intercourse during the treatment period to ensure the infection clears completely.
Antibiotics alone are successful in 34-75% of cases. Patients who do not improve in 72 hours are re-evaluated for laparoscopic or surgical intervention and for other possible diagnoses. Laparoscopy should be used if the diagnosis is in doubt. Laparoscopic pelvic lavage, abscess drainage, and adhesiolysis may be necessary. Laparoscopy gives direct visualization of internal organs and of the pelvis and obtaining of cultures for more accurate bacteriologic diagnosis. However, laparoscopy is not always available in acute PID; moreover, it is costly and requires general anesthesia.
If surgical treatment is required, attempt is to conserve reproductive potential with simple drainage, adhesiolysis, and copious irrigation or unilateral adnexectomy, if possible. Further surgical therapy is needed in 15-20% of cases so managed.
Most tubo-ovarian abscess (60-80%) resolve with antibiotic administration. Laparoscopy may be used to identify the loculations of pus requiring drainage. Unresolved abscesses may be drained by colpotomy, laparoscopy, or laparotomy. In patients with recurrent PID, dense pelvic adhesions may render surgery difficult.
Removal of intrauterine devices (IUDs) in acute PID cases is not necessary. But close clinical follow-up is mandatory if the IUD is left in place.
More research is needed to optimize PID diagnosis and treatment; and to improve patient and doctor’s compliance to guidelines.
COMPLICATIONS
Untreated PID may cause scar tissue, and collections of infected fluid (abscesses) in the fallopian tubes, which can damage the reproductive organs.
Other possible complications are:
• Ectopic pregnancy. The scar tissue prevents the fertilized egg from moving through the fallopian tube to implant in the uterus thus causing a tubal (ectopic) pregnancy that can cause massive, life-threatening bleeding and that may require emergency medical attention. PID is a major cause of ectopic pregnancy
• Infertility. PID may damage the reproductive organs and cause infertility. Delaying the treatment, or frequent PID, dramatically increases the risk of infertility. In the US, 1 in 8 women with a history of PID has difficulty getting pregnant; and 15% of infertility cases are because of PID.
• Chronic pelvic pain. Pelvic inflammatory disease can cause pelvic pain that may last for months or years. Scarring in fallopian tubes and other pelvic organs can cause pain during intercourse and ovulation.
• Tubo-ovarian abscess. PID might cause an abscess — a collection of pus — to form in uterine tube and ovaries. If left untreated, this could develop into a life-threatening infection.
PREVENTION
To reduce the risk of PID:
• Practice safe sex. Use condoms every time you have sex, limit your number of partners, and ask about a potential partner’s sexual history.
• Talk to your doctor about contraception. Many forms of contraception do not protect against the development of PID. Using barrier methods, such as a condom, might help to reduce your risk. Even if you take birth control pills, it’s still important to use a condom every time you have sex to protect against STIs.
• Get tested. If you’re at risk of an STI, such as chlamydia, make an appointment with your doctor for testing. Set up a regular screening schedule with your doctor if needed. Early treatment of an STI gives you the best chance of avoiding PID.
• Request that your partner be tested. If you have PID or an STI, advise your partner to be tested and, if necessary, treated. This can prevent the spread of STIs and possible recurrence of PID.
• Don’t douche. Douching upsets the balance of bacteria in your vagina.
INCIDENCE
In a 1995 U.S. study, 8 percent of all women in their reproductive years were being treated for PID. The numbers have steadily reduced. In 2015, the annual visits for PID were down to about 90,000 a year.
Enough data on incidence of PID in India is not available. In one study about 11.55% of the study subjects were diagnosed with PID. In the industrialised world, the incidence is 1 to 2 per cent per year among sexually active women. On that basis, India will have about one million PID cases per year.
REDUCING THE INCIDENCE
Because of difficulty of diagnosis, and serious consequences of delayed treatment, it is recommended that empirical treatment should be initiated in at-risk women who have lower abdominal pain, adnexal tenderness, and cervical motion tenderness. That overtreatment be preferred to no or delayed treatment.
Women with PID should be counselled to abstain from sexual activity or use barrier protection strictly and appropriately until their symptoms and those of their partner have fully abated and they have completed their entire treatment regimen.
Improved education, routine screening, diagnosis, and empirical treatment of PID will reduce the incidence and prevalence of PID and its long-term sequelae. Education should concentrate on strategies to prevent PID and STIs, including reducing the number of sexual partners, avoiding unsafe sexual practices, and routinely using appropriate barrier protection. Adolescents, being at an increased risk for PID, should be advised to delay the onset of sexual intercourse until age 16 years or older.